Coronavirus news #7. As always, please point out my errors. I started making notes a couple of weeks ago before getting side-tracked. In the meantime, we've had 2 million new reported cases - about 20% of the total.
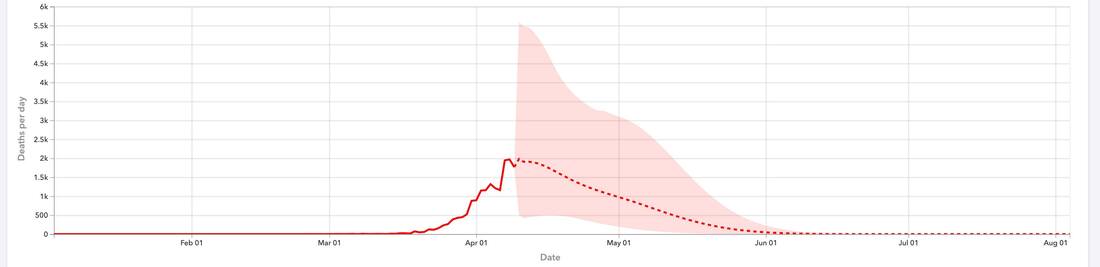
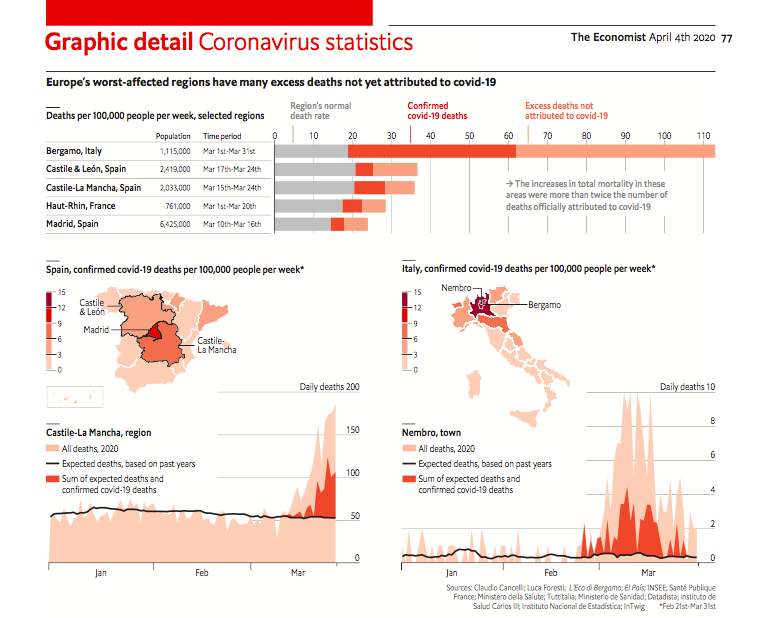
1) About 4000-5000 people are reported to die everyday because of this virus, or about 3% of all deaths. Globally, that has been stable for nearly 2 months. The true number is almost certainly higher, but it's unlikely to be by a whole lot (high uncertainty in India and some other places, though). Please remember that the people who don't die don't all recover completely. Many, many more are being struck with long-term damage to their health. That includes a substantial number that don't have any symptoms and may not even realise it now; many asymptomatic people show signs of lung damage in scans. So though it's normal to have one's standards for safety slip after all this time and with fewer immediate consequences in our daily lives, please be safe. Wear a mask.
2) Though the US mostly leads the news, Brazil and possibly Mexico are likely in worse shape, with India bidding to take this miserable crown. South Africa also seems fairly likely to join that group. Nobody really knows what's happening in Russia, because there's clear signs that some of the data being released are junk. Unlike the other countries, the US has actually been declining in deaths per day since the beginning of May. Brazil, Mexico, South Africa and India are still increasing, and the first two have substantially more daily deaths than the US. There has been a worrying drop-off in reporting (even by scientists) about the state of the virus in the developing world, with Brazil being a partial exception.
3) The US has seen explosive growth in cases in the last three weeks but deaths per day have actually declined since early May. There's multiple reasons for this. A greater proportion of new cases are in younger people (~10-100X less likely to die), we have developed better methods to manage severe illnesses, and perhaps most importantly, we are catching cases earlier. The last point implies that the lag between increases in cases and increases in deaths should be increasing. It used to be about 2 weeks; it may be 3 or 4 now. If this hypothesis is true, we should see increases in deaths across much of the US in another week or so. We can be fairly confident that the growth in cases is not simply because of more testing, because many of the outbreaks are also seeing an increase in the percentage of positive tests - a sign that an increasing number of cases is being missed.
4) Europe shouldn't feel too thrilled. After getting things under control, they've messed up the reopening and experienced about a month of increasing daily cases. Switzerland has finally mandated mask usage in public transportation. I think that ought to be the minimum policy change that we should aim for. There seems to be reasonable evidence that mandatory mask usage and closing some activities that involve crowds or closed spaces (e.g. bars) would be sufficient to kill the pandemic. Mask usage alone does a lot of the heavy lifting. Even tighter restrictions would do it faster but might be overkill if the situation is not yet out of control.
5) Antibodies are the focus of 2 important types of testing: (i) testing to figure out if someone has had the disease and will therefore be immune, and (ii) testing to figure out what proportion of the population has been infected by the disease ('seroprevalence studies'). This is how we get exposed/infected numbers like 5% of the Spanish population (it's similar in the US). But we now know that antibodies actually decay below our ability to detect them relatively fast, roughly on the scale of months. This does not mean that these people have lost immunity; they almost certainly retain the ability to produce more antibodies in the future if re-infected by the virus. Also, some indeterminate (but probably low) number of people apparently tend to not show much of an antibody response. However, most (if not all) people develop another type of immunity that is mediated by specialised T-cells. These provide long-term immunity and are generally ignored because they are much harder to test for. They are not quite as effective as antibodies but are likely important, though we don't know much about their role in COVID immunity yet. Bottom line: (a) we are still fairly confident that people develop immunity after infection, (b) the antibodies we test for decrease over time but we retain immunity, (c) this antibody decrease & T-cell response adds an unknown but probably small bias to our estimates of how much of the population has been exposed.
6) There appears to be some pre-existing immunity in people who were infected by SARS-1 many years ago and by an unknown coronavirus. There are 7 documented coronaviruses circulating in human populations, but there is likely an unknown one circulating in South-East Asia that has protected populations there through this 'cross-immunity'.
7) Most evidence points towards us being very far from any sort of herd immunity. If the governments of the US, India & Brazil give up on containing this, I would say we are heading towards millions of deaths with high probability (given their failure so far, we are headed there already with moderate probability). To speculate even further, tens of millions is not implausible in this scenario.
8) Last month, I wrote that perhaps 80% of new cases are caused by 10% of infected people (superspreaders). This has important implications for how to do contact tracing. The standard method is to find everyone an infected person was in contact with and notify/quarantine them. But since they were almost certainly infected by a superspreader, an improvement on this is to identify the superspreader who passed it to them and then trace everyone they were in contact with. This 'backward contact tracing' can be thought of as a second level that makes the whole procedure much more effective at stopping an outbreak. That said, contact tracing isn't feasible when you have a massive ongoing outbreak.
9) There is now plausible but inconclusive evidence that the virus has adapted during its spread. A mutation that increases the spread in limited lab experiments has also come to dominate in new cases around the world in the last 3-4 months. But it could have spread more just by chance, by being in the first cases that spread to new places. However, the mutation does not appear to do anything to the virus' lethality, so this evolution has not made things any better for us. And it does not change anything about how we should prepare for or treat it.
10) Despite all the press about treatments, no specific medication we have so far is close to being a cure. Hydroxychloroquine does not do much and has wasted time and money. Remdesivir and Dexamethasone have relatively weak effects or limited use-cases; they will save lives but are not cures. When used most effectively, dexamethosone appears to save about 25% of lives lost. This is progress, but we need a lot better. Both also have severe, dangerous side-effects that can kill. We are on the way to having monoclonal antibody treatments, probably within a few months. This would be a big improvement but is probably going to be expensive. The US appears to be doing its best to corner the market on these right now, though that investment should stimulate more development.
11) Children appear to be about 1/3 to 1/2 as likely to get infected. And they are much less likely to fall seriously ill or die once infected; they have ~100X lower probability of dying if infected, relative to people over 80. This has obvious implications for reopening schools and colleges. I think doing so is probably feasible if coupled with distancing, mandatory masking, and mass testing on a regular basis to catch outbreaks early. But the details matter a lot.
12) There's now even more evidence that surfaces are not that important for spreading the virus.
-----------------
In response to a question about whether we were headed in the right direction at this time:
Absolutely in the wrong direction in the US right now.
We still don't have enough tests or protective equipment, mask usage is not high enough, people in outbreak areas appear to still be frequenting indoor restaurants (less than normal, but still), new cases are going up rapidly, and the federal government & the CDC continue to be disastrous (more on that soon).
The main good news is that deaths per day are much lower than May, but as I said above, I expect that to increase soon. There's a phenomenal amount of scientific talent, of course, but it's not much good if the people in charge are incompetent, malicious or craven (or some combination of the above).
Other that that, the prospect of monoclonal antibodies, some advances on treatment, and some progress on the vaccine front are all encouraging. But none of them is close to deployment.
1) About 4000-5000 people are reported to die everyday because of this virus, or about 3% of all deaths. Globally, that has been stable for nearly 2 months. The true number is almost certainly higher, but it's unlikely to be by a whole lot (high uncertainty in India and some other places, though). Please remember that the people who don't die don't all recover completely. Many, many more are being struck with long-term damage to their health. That includes a substantial number that don't have any symptoms and may not even realise it now; many asymptomatic people show signs of lung damage in scans. So though it's normal to have one's standards for safety slip after all this time and with fewer immediate consequences in our daily lives, please be safe. Wear a mask.
2) Though the US mostly leads the news, Brazil and possibly Mexico are likely in worse shape, with India bidding to take this miserable crown. South Africa also seems fairly likely to join that group. Nobody really knows what's happening in Russia, because there's clear signs that some of the data being released are junk. Unlike the other countries, the US has actually been declining in deaths per day since the beginning of May. Brazil, Mexico, South Africa and India are still increasing, and the first two have substantially more daily deaths than the US. There has been a worrying drop-off in reporting (even by scientists) about the state of the virus in the developing world, with Brazil being a partial exception.
3) The US has seen explosive growth in cases in the last three weeks but deaths per day have actually declined since early May. There's multiple reasons for this. A greater proportion of new cases are in younger people (~10-100X less likely to die), we have developed better methods to manage severe illnesses, and perhaps most importantly, we are catching cases earlier. The last point implies that the lag between increases in cases and increases in deaths should be increasing. It used to be about 2 weeks; it may be 3 or 4 now. If this hypothesis is true, we should see increases in deaths across much of the US in another week or so. We can be fairly confident that the growth in cases is not simply because of more testing, because many of the outbreaks are also seeing an increase in the percentage of positive tests - a sign that an increasing number of cases is being missed.
4) Europe shouldn't feel too thrilled. After getting things under control, they've messed up the reopening and experienced about a month of increasing daily cases. Switzerland has finally mandated mask usage in public transportation. I think that ought to be the minimum policy change that we should aim for. There seems to be reasonable evidence that mandatory mask usage and closing some activities that involve crowds or closed spaces (e.g. bars) would be sufficient to kill the pandemic. Mask usage alone does a lot of the heavy lifting. Even tighter restrictions would do it faster but might be overkill if the situation is not yet out of control.
5) Antibodies are the focus of 2 important types of testing: (i) testing to figure out if someone has had the disease and will therefore be immune, and (ii) testing to figure out what proportion of the population has been infected by the disease ('seroprevalence studies'). This is how we get exposed/infected numbers like 5% of the Spanish population (it's similar in the US). But we now know that antibodies actually decay below our ability to detect them relatively fast, roughly on the scale of months. This does not mean that these people have lost immunity; they almost certainly retain the ability to produce more antibodies in the future if re-infected by the virus. Also, some indeterminate (but probably low) number of people apparently tend to not show much of an antibody response. However, most (if not all) people develop another type of immunity that is mediated by specialised T-cells. These provide long-term immunity and are generally ignored because they are much harder to test for. They are not quite as effective as antibodies but are likely important, though we don't know much about their role in COVID immunity yet. Bottom line: (a) we are still fairly confident that people develop immunity after infection, (b) the antibodies we test for decrease over time but we retain immunity, (c) this antibody decrease & T-cell response adds an unknown but probably small bias to our estimates of how much of the population has been exposed.
6) There appears to be some pre-existing immunity in people who were infected by SARS-1 many years ago and by an unknown coronavirus. There are 7 documented coronaviruses circulating in human populations, but there is likely an unknown one circulating in South-East Asia that has protected populations there through this 'cross-immunity'.
7) Most evidence points towards us being very far from any sort of herd immunity. If the governments of the US, India & Brazil give up on containing this, I would say we are heading towards millions of deaths with high probability (given their failure so far, we are headed there already with moderate probability). To speculate even further, tens of millions is not implausible in this scenario.
8) Last month, I wrote that perhaps 80% of new cases are caused by 10% of infected people (superspreaders). This has important implications for how to do contact tracing. The standard method is to find everyone an infected person was in contact with and notify/quarantine them. But since they were almost certainly infected by a superspreader, an improvement on this is to identify the superspreader who passed it to them and then trace everyone they were in contact with. This 'backward contact tracing' can be thought of as a second level that makes the whole procedure much more effective at stopping an outbreak. That said, contact tracing isn't feasible when you have a massive ongoing outbreak.
9) There is now plausible but inconclusive evidence that the virus has adapted during its spread. A mutation that increases the spread in limited lab experiments has also come to dominate in new cases around the world in the last 3-4 months. But it could have spread more just by chance, by being in the first cases that spread to new places. However, the mutation does not appear to do anything to the virus' lethality, so this evolution has not made things any better for us. And it does not change anything about how we should prepare for or treat it.
10) Despite all the press about treatments, no specific medication we have so far is close to being a cure. Hydroxychloroquine does not do much and has wasted time and money. Remdesivir and Dexamethasone have relatively weak effects or limited use-cases; they will save lives but are not cures. When used most effectively, dexamethosone appears to save about 25% of lives lost. This is progress, but we need a lot better. Both also have severe, dangerous side-effects that can kill. We are on the way to having monoclonal antibody treatments, probably within a few months. This would be a big improvement but is probably going to be expensive. The US appears to be doing its best to corner the market on these right now, though that investment should stimulate more development.
11) Children appear to be about 1/3 to 1/2 as likely to get infected. And they are much less likely to fall seriously ill or die once infected; they have ~100X lower probability of dying if infected, relative to people over 80. This has obvious implications for reopening schools and colleges. I think doing so is probably feasible if coupled with distancing, mandatory masking, and mass testing on a regular basis to catch outbreaks early. But the details matter a lot.
12) There's now even more evidence that surfaces are not that important for spreading the virus.
-----------------
In response to a question about whether we were headed in the right direction at this time:
Absolutely in the wrong direction in the US right now.
We still don't have enough tests or protective equipment, mask usage is not high enough, people in outbreak areas appear to still be frequenting indoor restaurants (less than normal, but still), new cases are going up rapidly, and the federal government & the CDC continue to be disastrous (more on that soon).
The main good news is that deaths per day are much lower than May, but as I said above, I expect that to increase soon. There's a phenomenal amount of scientific talent, of course, but it's not much good if the people in charge are incompetent, malicious or craven (or some combination of the above).
Other that that, the prospect of monoclonal antibodies, some advances on treatment, and some progress on the vaccine front are all encouraging. But none of them is close to deployment.